Background and Need
The mitral valve is a two-leaflet valve and is the passageway between the left atrium and the left ventricle of the heart. The chordae tendineae are tendon-like chords that anchor the mitral valve leaflets to the papillary muscles. The chords prevent the leaflets from mitral valve prolapse into the left atrium. Mitral regurgitation happens when the mitral valve does not close completely and there is retrograde blood flow into the left atrium. When there is retrograde flow in the heart, the blood flow does not move efficiently through the heart, which reduces cardiac output and can make you feel tired or out of breath. (6)
Mitral regurgitation is the most common form of valvular heart disease. Two percent of the adult population suffers from mitral regurgitation with similar prevalence in males and females. There are 20 to 25 thousand mitral valve procedures performed a year with an 80% success rate. (6) However, only 44.3% of patients who have mitral regurgitation actually undergo mitral valve repair. This is due to the high complexity of the surgery and risk factors associated with the operations. Symptomatic patients have an annular death rate of 5% or more without intervention. (4)
In the United States degenerative mitral valve disease is the most common cause of mitral regurgitation. (7) Detached or elongated chordae of the posterior leaflet are the most common sources for mitral regurgitation. (13) Mitral valve regurgitation is most often mild and progresses slowly. Severe mitral valve regurgitation can lead to heart failure, atrial fibrillation, endocarditis, and pulmonary hypertension. There is a positive feedback loop associated with mitral regurgitation. Mild mitral regurgitation leads to less blood flow in the body, which leads to less oxygen circulation. Receptors in the heart sense the lack of oxygen flow and therefore dilate the annulus of the valve. This leads to poorer valvular function, which in turn leads to a greater retrograde flow in the heart, which increasingly contributes to the positive feedback loop. Therefore valvular repair should be recommended for patients with mild mitral regurgitation because the condition will become progressively worse with time. (1) However, currently the guidelines recommend surgery for moderate-to-severe or severe mitral regurgitation in patients with symptoms or indication of left ventricular dysfunction. (4)
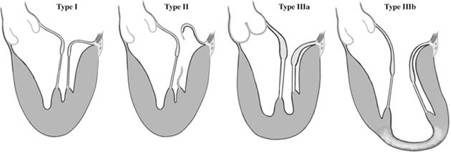
There are three types of mitral regurgitation, shown in Figure 1. Type I is when the valve is enlarged and is caused by annular dilation. Type I regurgitation is quite rare and requires valvular replacement or annuloplasty. Type II, or mitral valve prolapse, is when there is increased leaflet motion; it is the most common form of MR. There are different subtypes of Type II regurgitation. Type IIa occurs when the chordae tendineae stretch out and type IIb occurs when the chordae tendineae rupture. Type IIc occurs when the papillary muscle scars and Type IId occurs when the papillary muscle ruptures. Minimal invasive catheter repairing of Type II mitral regurgitation is what we are focusing on for our design project. Type III regurgitation occurs with restricted leaflet motion. (1)
Figure 1: Type I: Normal mitral motion
Type II: Increased leaflet motion
Type IIIa: Restricted leaflet motion during diastole and systole
Type IIIb: Restricted leaflet motion predominantly during systole
Mitral regurgitation is the most common form of valvular heart disease. Two percent of the adult population suffers from mitral regurgitation with similar prevalence in males and females. There are 20 to 25 thousand mitral valve procedures performed a year with an 80% success rate. (6) However, only 44.3% of patients who have mitral regurgitation actually undergo mitral valve repair. This is due to the high complexity of the surgery and risk factors associated with the operations. Symptomatic patients have an annular death rate of 5% or more without intervention. (4)
In the United States degenerative mitral valve disease is the most common cause of mitral regurgitation. (7) Detached or elongated chordae of the posterior leaflet are the most common sources for mitral regurgitation. (13) Mitral valve regurgitation is most often mild and progresses slowly. Severe mitral valve regurgitation can lead to heart failure, atrial fibrillation, endocarditis, and pulmonary hypertension. There is a positive feedback loop associated with mitral regurgitation. Mild mitral regurgitation leads to less blood flow in the body, which leads to less oxygen circulation. Receptors in the heart sense the lack of oxygen flow and therefore dilate the annulus of the valve. This leads to poorer valvular function, which in turn leads to a greater retrograde flow in the heart, which increasingly contributes to the positive feedback loop. Therefore valvular repair should be recommended for patients with mild mitral regurgitation because the condition will become progressively worse with time. (1) However, currently the guidelines recommend surgery for moderate-to-severe or severe mitral regurgitation in patients with symptoms or indication of left ventricular dysfunction. (4)
There are three types of mitral regurgitation, shown in Figure 1. Type I is when the valve is enlarged and is caused by annular dilation. Type I regurgitation is quite rare and requires valvular replacement or annuloplasty. Type II, or mitral valve prolapse, is when there is increased leaflet motion; it is the most common form of MR. There are different subtypes of Type II regurgitation. Type IIa occurs when the chordae tendineae stretch out and type IIb occurs when the chordae tendineae rupture. Type IIc occurs when the papillary muscle scars and Type IId occurs when the papillary muscle ruptures. Minimal invasive catheter repairing of Type II mitral regurgitation is what we are focusing on for our design project. Type III regurgitation occurs with restricted leaflet motion. (1)
Figure 1: Type I: Normal mitral motion
Type II: Increased leaflet motion
Type IIIa: Restricted leaflet motion during diastole and systole
Type IIIb: Restricted leaflet motion predominantly during systole
Project Scope
Mitral regurgitation is the most common form of valvular heart disease. Our project is the final step in a three-step process to repair Type II Mitral Regurgitation (MR). The first step was to attach an artificial chordae to the mitral leaflet. The second step was to attach a separate chordae to the left ventricle wall. Our project is to adjust the lengths of the chordae and to cinch them together.
Previous techniques for MR repair have involved putting the patient through cardiac bypass and using cardioplegia to stop the patient’s heart in order to repair the mitral valve. For our project, we aim to use a minimally invasive procedure that will be preformed while the patient is under general anesthesia and the heart is still beating. This would create radical changes in the way mitral valves are repaired. Our goal is to use a minimally invasive transfemoral catheter-based approach to enter the heart and repair the damaged mitral valve.
There is a large market for this type of procedure because degenerative diseases are a growing issue as life expectancy increases. MR is one of the top two valvular diseases, affecting 2% of the population. Our system would be competitive and advanced for the current market because our procedure involves less risk and side effects than procedures using cardioplegeia.
We plan on shadowing cardiologists performing MR repair. We hope to design a product that incorporates clinical technique to maintain the physiology of the heart and is also within the restrictions of engineering. We will use CAD to make detailed designs of our system and then consult with experts in the manufacturing field about our development time, process, and cost. If this design proves to be profitable, we will submit our design and report to investors, doctors, and existing medical device companies.
Previous techniques for MR repair have involved putting the patient through cardiac bypass and using cardioplegia to stop the patient’s heart in order to repair the mitral valve. For our project, we aim to use a minimally invasive procedure that will be preformed while the patient is under general anesthesia and the heart is still beating. This would create radical changes in the way mitral valves are repaired. Our goal is to use a minimally invasive transfemoral catheter-based approach to enter the heart and repair the damaged mitral valve.
There is a large market for this type of procedure because degenerative diseases are a growing issue as life expectancy increases. MR is one of the top two valvular diseases, affecting 2% of the population. Our system would be competitive and advanced for the current market because our procedure involves less risk and side effects than procedures using cardioplegeia.
We plan on shadowing cardiologists performing MR repair. We hope to design a product that incorporates clinical technique to maintain the physiology of the heart and is also within the restrictions of engineering. We will use CAD to make detailed designs of our system and then consult with experts in the manufacturing field about our development time, process, and cost. If this design proves to be profitable, we will submit our design and report to investors, doctors, and existing medical device companies.
